
LONG COVID KIDS RESPONSE TO THE JCVI MINUTES ON CHILD VACCINES
- Long Covid Kids

- Nov 6, 2021
- 4 min read
Updated: Sep 27, 2025
LCK Representative for Scotland
After months of silence, on Friday 29th October the Joint Committee on Vaccination and Immunisation (JCVI) released the long-awaited minutes of meetings held on discussions surrounding child COVID19 vaccinations.
The meeting minutes caused outrage on social media from scientists, healthcare professionals and the public. Not only because of the disappointing content, but also because the minutes of multiple meetings since May 2021 were published at the same time. This has sparked upset that JCVI may have sat on the unpublished minutes for quite some time before releasing them to the public.
Minutes from a meeting held on Thursday 13th May outline the JCVIs arguments against vaccination in children.

The Long Covid Kids team were disappointed to read the minutes of the meetings and responded with a statement,
Long Covid Kids Data Analyst, James Neil ran the JCVI's own data and discovered a 360% direct benefit of vaccination that the JCVI had seemingly ignored.
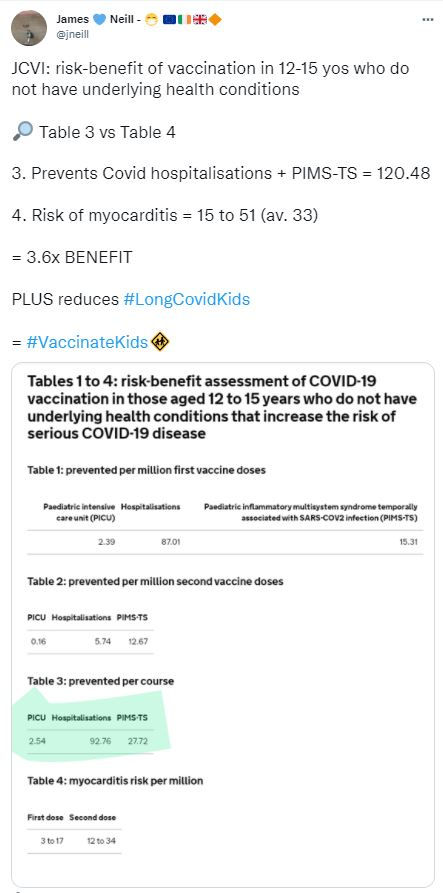
Here's the workings on the 360% direct benefit (i.e. x3.6) using JCVI's own data:
JCVI risk-benefit of vaccination in 12-15 yos who do not have underlying health conditions
Table 3 is hospitalisations prevented by course of vaccination
Add Covid hospitalisations, 92.76, and PIMS-TS, 27.72, to get 120.48 total hospitalisations
Table 4 is myocarditis risk from vaccination
Total risk of myocarditis = 15 to 51 giving an average of 33
120.48 / 33 = 3.65

James summarized, "so a course of child Covid vaccinations has a 365% (I rounded down to 360%) direct benefit to healthy children vs the risk of myocarditis".
"Also it's worth noting their myocarditis risk was for all children, not just "healthy" (i.e. without pre-existing conditions)"
So not an apples for apples comparison anyway.
An article in the Guardian newspaper echoed James' findings.

Twitter reactions to the JCVI minutes:

Professor Christina Pagel, Professor of Operational Research at University College London (UCL) and Director of the UCL Clinical Operational Research Unit.
"Two models from Warwick and PHE showed "substantial reduction in hospitalisations of 12-17 year olds".
Both models estimated vax would prevent 3 deaths per million kids vaxxed. (2/million in prev healthy children). Warwick also showed LARGE REDUCTION in INFECTIONS. The JCVI remained unmoved. They thought opportunity costs (affecting school vax progs) & potential harms from vax (although they earlier acknowledged vax myocarditis was q mild) outweighed benefit (but no numbers to support). They also touted natural infection as better *again*
They then dismissed PIMS-TS (severe rare syndrome in kids than puts many in ICU) and Long Covid as rare. But rare with high number of infections can be significant. AND vax causes neither - so benefits here must outweigh risk - esp as vax WILL REDUCE OVERALL INFECTIONS IN KIDS.
Depsite frequently saying education not their remit, they somewhat strangely seem to say that kids getting covid is less disruptive to education (or should be less disruptive?) than vaccination?!
In 1st July minutes (pt 7), JCVI say they didn't trust the modelling because it was based on wave 2 when adults weren't vaxxed. They believed that high vax rates in adults would stop cases in children I think. We can see how that turned out.
There is much more to say about the minutes & the contradictory statements that appear throughout (esp on remit). But these bits show they had modelling showing significant benefit and just dismissed it. They worried so much about vax myocarditis & so little about covid."

Professor Colin Davies, chair in Cognitive Psychology at Bristol University.
""Children rarely develop severe disease or die of COVID-19; even children with underlying comorbidities have a very low risk."
Really?
Over 10,000 children have been hospitalised in UK.
Over 100 children have died.
Over 10,000 have been ill for over a year (ONS estimate).
"There are limited data on COVID-19 vaccine use in children; there is a need to consider the mild transient illness of COVID-19 versus potential rare adverse events associated with vaccination."
The vaccine is safe and effective. COVID in children isn't always mild or transient.
"All adults will be vaccinated and there is a low risk of child-to-child transmission. Staff and parents will be protected."
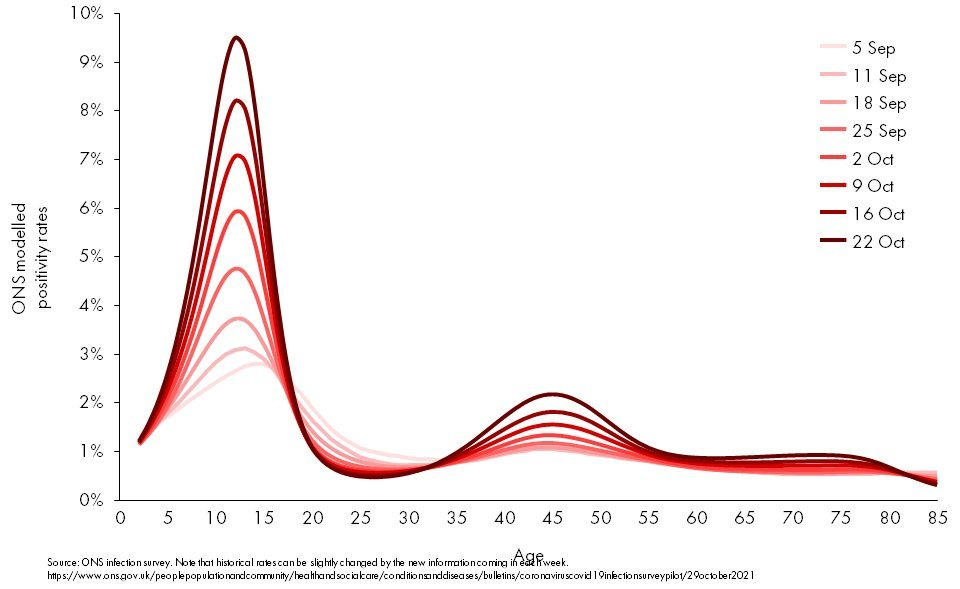
Children infect each other - a lot. They also infect vaccinated adults: teachers & parents. (graph: @PaulMainwood)
"Childhood infections reflect adult infection in the community; vaccinating adults will lead to lower community infection rates and lower risk of transmission to children."
Nope. Transmission in schools drives the epidemic (especially when adults are mostly vaccinated).
"There is an argument for allowing the virus to circulate amongst children which could provide broader immunity to the children and boost immunity in adults."
And here we have it: #HerdImmunityViaMassInfection"

Deepti Gurdasani, clinical epidemiologist and Senior lecturer in Machine Learning at Queen Mary University of London retweeting a thread from Karam Bales, NEU National Executive. Chair of NP&YW National Council.
"I would expect this from anti-vaxx groups, not a scientific committee."

Kit Yates, Mathematical Biologist at the University of Bath.
LongCovidKids.org is a UK based international charity supporting and advocating for families, children and young people living with Long Covid. Our story started with a short film on the long-lasting symptoms of Covid in children.
Each Sunday we send out a newsletter providing a weekly round-up of statistics, the latest reports in the media, current research, and LCK news. Read previous issues and SIGN UP
Please donate to help us keep raising awareness, LCK is run by volunteers. Your support enables us to support families worldwide.


